PTSD Still Has No Blood Biomarker. A Biobank Study Shows Why That Might Change.
Apr 12, 2026
Thirty years of research on PTSD biology has produced a long list of candidate biomarkers and almost no diagnostics. A new paper in Molecular Psychiatry uses a health system biobank to triangulate genomic signals, routine lab values, and clinical phenotypes at scale. The finding is less about any single candidate and more about the operating model: psychiatric biomarker discovery is finally getting infrastructure worthy of the problem.
Thirty years of research on PTSD biology has produced a long list of candidate biomarkers and almost no diagnostics. Elevated interleukin-6, low baseline cortisol, dysregulated glucocorticoid receptor sensitivity, altered HPA axis signaling: each finding has appeared in multiple studies, and none has survived replication consistently enough to anchor a clinical test.
The failure is not entirely about the biology. It is partly about how the research has been organized: small cohorts, inconsistent phenotyping, and no shared infrastructure for moving from discovery to validation. A paper published in Molecular Psychiatry argues that health system biobanks can change this, not by finding a magic biomarker, but by building a more defensible operating model for hunting one.
The Graveyard of Replication
The neuroinflammation hypothesis for PTSD has real support. A 2022 review in Biomedicines documented consistently elevated inflammatory biomarkers in PTSD patients, including IL-1, IL-6, TNF-alpha, and C-reactive protein, alongside HPA axis changes that appear to cross the blood-brain barrier and trigger neuroinflammatory cascades in limbic and prefrontal regions. The biology is plausible, mechanistically coherent, and supported by animal models. The problem is that plausible biology does not produce a useful diagnostic on its own.
Inflammatory markers are not specific to PTSD. IL-6 is elevated in depression, chronic pain, cardiovascular disease, and obesity. Cortisol is sensitive to time of day, recent stressors, and medication. When a study of 80 patients versus 80 controls finds a statistically significant association, the effect size is inflated relative to what would be found in a larger, more representative sample. When the next lab tries to replicate it in a different population with a slightly different phenotype definition, the signal often shrinks or disappears. The literature is full of biomarker candidates that looked promising in one paper and failed in the next three.
PTSD is a particularly difficult case because the clinical phenotype is inherently variable. Trauma exposure is heterogeneous. Symptom presentation shifts over time. DSM criteria can be applied differently across clinicians and settings. Two patients sharing a PTSD diagnosis may have substantially different underlying biology. Running a biomarker study in this context, with a small and loosely characterized sample, is not a reliable way to find findings that travel.
The Infrastructure Problem
The structural issue is that psychiatric biomarker research has mostly been conducted at the wrong scale, with tools poorly suited to the noise level of the phenotype. Jordan Smoller at Harvard published a foundational review in 2018 on the use of electronic health records for psychiatric phenotyping and genomics. His analysis showed that curated EHR-derived phenotypes for psychiatric conditions can achieve high positive predictive values (above 0.90 in well-developed algorithms), and that linking EHR data to biospecimens and genomics could directly address the sample size constraints that have limited genetic research in psychiatry for decades.
The operative word is curated. Raw diagnostic codes applied to a health system EHR are noisy. For PTSD specifically, ICD coding is inconsistent across care settings, trauma histories are poorly documented in structured fields, and patients seen primarily for comorbidities may be underdiagnosed or incorrectly coded. Building a reliable PTSD phenotype from EHR data requires integrating medication records, symptom assessment scores, and sometimes clinical notes. That is a substantial investment. Most academic psychiatric research programs have not made it at the scale required for genome-wide biomarker discovery.
The result has been a field of adequately powered epidemiological studies that cannot generate the sample sizes needed for robust genomic analysis. The VA Million Veteran Program changed the calculus for one large population. A 2021 Nature Genetics paper on genome-wide association analyses of PTSD in more than 250,000 MVP participants identified multiple genome-wide significant loci and demonstrated that PTSD shares genetic architecture with mood and anxiety disorders. That study set a new bar for what psychiatric genomics can produce when the infrastructure is properly built. The question the Molecular Psychiatry paper takes up is whether that discovery infrastructure can be extended to laboratory biomarker work.
What the Biobank Adds
The paper applies a method called a laboratory-wide association study (LabWAS) to PTSD in a health system biobank. The LabWAS approach was formalized in a 2020 PLOS Genetics paper by Goldstein and colleagues at Northwestern, Michigan, and Vanderbilt, using data from BioVU and the Michigan Genomics Initiative. Instead of pre-specifying candidate biomarkers, a LabWAS scans thousands of routine clinical lab values simultaneously for genetic associations, letting the data surface candidates systematically across the full measurement space captured in the EHR. The method is designed for biobank-linked genomic data where you have both genetic information and longitudinal lab records for tens of thousands of patients.
The triangulation in the Molecular Psychiatry paper uses two distinct exposures. The first is clinical PTSD diagnosis derived from EHR phenotyping. The second is a PTSD polygenic risk score (PRS) constructed from the MVP GWAS and applied to biobank participants. The use of two exposures matters because they have different confounding structures. Clinical diagnosis is affected by treatment history, comorbidity burden, and phenotyping algorithm decisions. The PRS is a genomic measure, independent of medication and less susceptible to diagnostic noise. Lab values that associate with both exposures, consistently and in the same direction, carry stronger prior probability of reflecting true PTSD biology than values associating with only one.
The value of PRS as an exposure here is underscored by recent longitudinal work. A 2025 Molecular Psychiatry study following 5,687 World Trade Center responders over 20 years found that PTSD polygenic risk significantly predicted long-term symptom trajectories: higher PRS was associated with more rapid symptom increases and steeper long-term clinical courses. When a genomic signal predicts clinical outcomes across two decades of prospective follow-up, associations it surfaces in a LabWAS become more credible starting hypotheses.
Reading the Signal Map
The triangulation scanned lab values across eight physiological systems: cardiometabolic (55 measures), endocrine (21), genitourinary (22), hematologic (53), hepatic (10), immune (61), a residual other category (9), and toxicology and pharmacology (10). After Bonferroni correction for multiple comparisons, statistically significant associations clustered most prominently in the immune and hematologic categories, with additional signals in cardiometabolic measures. The pattern aligns with the neuroinflammation literature but is now grounded in a much larger, more systematically phenotyped dataset than most prior work in the field.
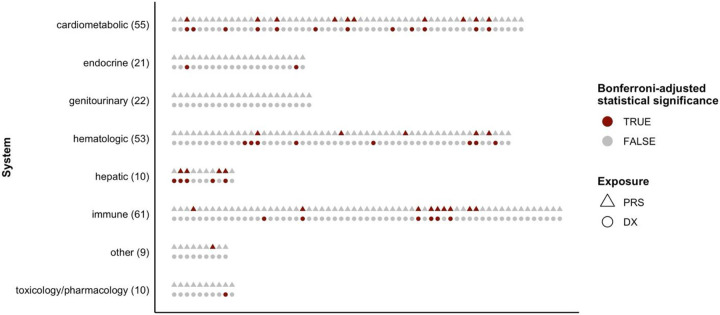
What the figure makes clear is that no single physiological system dominates. Signals are distributed across immune, hematologic, and cardiometabolic categories, and the significant hits appear in both the PRS and diagnosis exposure arms for some lab values. This is consistent with the current view of PTSD as a systemic condition, not a purely CNS disorder. The HPA axis, the immune system, and the cardiovascular system are all implicated, and they interact. A single biomarker is unlikely to be specific enough to function as a standalone diagnostic. A panel anchored by signals with convergent genomic and phenotypic support is a more realistic clinical target, and the triangulation framework is designed specifically to produce candidates of that quality.
The paper is also notable for what it does not claim. It does not present any individual lab value as a validated PTSD biomarker. It presents a ranked candidate landscape, ordered by evidence quality rather than p-value alone. That kind of epistemic restraint is not common in psychiatric biomarker literature, and it is the right call here.
What This Doesn't Mean
The Molecular Psychiatry paper is a discovery study. The lab associations it surfaces are hypotheses, not validated biomarkers. The path from a LabWAS hit to a deployable diagnostic runs through independent replication, analytical validation, clinical validation in prospective cohorts with structured phenotyping, and regulatory review. For a psychiatric condition with as much inherent phenotyping noise as PTSD, that path is longer than average. Most candidates will not survive it.
The EHR-based phenotyping also has limits even when done carefully. Smoller's review notes that EHR phenotypes for psychiatric conditions achieve high predictive values in well-developed algorithms, but imperfect. Patients miscoded, seen primarily for comorbidities, or inconsistently documented across care settings introduce noise. The biobank phenotype is a large-scale approximation of clinical diagnosis, useful for discovery and for generating prior probabilities, but not a substitute for structured research interviews in a validation study. Any candidate that advances should be retested in a cohort phenotyped at higher resolution before it becomes an assay development investment.
The Operating Model Is the Contribution
The most important output of this paper is not the candidate list. It is the demonstration that a health system biobank, linked to genomic data and EHR lab records, can generate a more defensible starting point for psychiatric biomarker discovery than any individual cohort study could produce. The triangulation of PRS and clinical diagnosis exposures against a comprehensive lab-value scan is a replicable workflow, not a one-off analysis. That is what makes it worth paying attention to.
Cardiovascular biomarker research accelerated when it gained access to large longitudinal cohorts, Framingham, UK Biobank, the Million Veteran Program, that linked biological measurements to years of clinical outcomes and genomic data. Psychiatric research is building equivalent infrastructure now, and PTSD is emerging as a productive test case: high clinical need, historically underserved by biomarker work, and now addressable at the scale that makes systematic genomic triangulation viable.
If this operating model is adopted more broadly, the discovery phase of psychiatric biomarker research becomes faster, cheaper, and more reproducible. The validation phase remains hard. But it is considerably easier to justify the cost of clinical validation when your candidate has genomic support, phenotypic triangulation across two independent exposure measures, and a large-scale discovery study behind it than when it emerged from a 60-person pilot that happened to clear a p-value threshold. Psychiatric disorders have needed this kind of platform for a long time. Watch carefully what comes out of it next.
References
- Towards scalable biomarker discovery in posttraumatic stress disorder: triangulating genomic and phenotypic evidence from a health system biobank. Molecular Psychiatry (2025). doi:10.1038/s41380-026-03553-z. PMC11888531.
- Lee, H. et al. (2022). Neuroinflammation in Post-Traumatic Stress Disorder. Biomedicines, 10(5), 953. PMC9138406.
- Smoller, J.W. (2018). The Use of Electronic Health Records for Psychiatric Phenotyping and Genomics. American Journal of Medical Genetics Part B, 177(7), 601-612. PMC6440216.
- Goldstein, J.A. et al. (2020). LabWAS: Novel findings and study design recommendations from a meta-analysis of clinical labs in two independent biobanks. PLOS Genetics, 16(11), e1009077. PMC7682892.
- Genome-wide association analyses of post-traumatic stress disorder and its symptom subdomains in the Million Veteran Program (2021). Nature Genetics, 53, 174-184. PMC7972521.
- Polygenic Risk and Exposure Severity Predict Trajectories of PTSD: A Prospective Cohort Study (2025). Molecular Psychiatry. PMID: 40973784.
Have questions about this research or our products?
Contact Our TeamGet new posts delivered to your inbox